
Abstract
Background
The risk of anti-tuberculosis (TB) drug-induced liver injury (DILI) in patients with chronic viral hepatitis (CVH) is not clear. The aim of this study was to investigate incidence and risk factors associated with TB DILI in CVH and non-CVH patients.
Methods
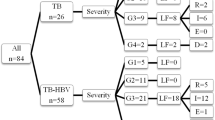
Retrospectively, a total of 128 CVH patients who received anti-TB medication from January 2005 to February 2014 were reviewed. Among these, 83 patients had hepatitis B virus (HBV), 41 patients had hepatitis C virus (HCV) and 4 patients were dual hepatitis B and hepatitis C virus co-infected (HBV + HCV) with 251 non-CVH patients who received anti-TB medication selected as the controls. There were no human immunodeficiency virus co-infected patients. Risk factors for DILI were analyzed using cox regression analysis.
Results
The incidence of DILI was significantly higher in the HCV group (13/41 [31.7 %], p < 0.001) and HBV + HCV groups (3/4 [75.0 %], p = 0.002) compared to the control group (25/251 [10.0 %]). The incidence of transient liver function impairment in the hepatitis B virus group was higher than in the control group (18/83 [21.7 %] vs. 27/251 [10.8 %] p = 0.010), but not in DILI (11/83 [13.3 %] vs. 25/251 [10.0 %], p = 0.400). In total patients, HCV, HBV + HCV co-infection, older age, and baseline liver function abnormality were independent factors of DILI.
Conclusions
It is recommended to carefully monitor for DILI in patients with HCV or HBV/HCV co-infection, older age, and baseline liver function abnormality.
Similar content being viewed by others

Background
Standard anti-tuberculosis (TB) drugs, including isoniazid (INH), rifampin (RFP), ethambutol (EMB), and pyrazinamide (PZA) are highly effective in treating TB. However, drug induced liver injury (DILI) associated with anti-TB treatment is the most important adverse event, which results in a low treatment success rate [1]. The incidence of DILI during standard anti-TB treatment ranges from 2 % to 28 % [2–6]. Once DILI occurs, all anti-TB drugs should be withheld until a complete resolution of the hepatotoxicity is accomplished [7]. Advanced age, female gender, alcohol abuse, malnutrition, and underlying chronic liver disease have been reported to be significant risk factors for DILI during anti-TB treatment [8–10]. However, it remains unclear whether the incidence of DILI increases during anti-TB treatment in patients with chronic viral hepatitis (CVH). In a previous Hong Kong study [11], persistent liver dysfunction was shown to be more common in hepatitis B virus (HBV) infected patients. In addition, several recent studies have suggested that HCV infections are also a significant risk factor for incident DILI during anti-TB treatment [12–15]. However, in still other studies, the incidence of transient liver dysfunction during anti-TB treatment was found to be higher in HBV or HCV infected patients than in patients without viral hepatitis, but the incidence of DILI was not different between CVH and non-CVH patients [16–20].
In Korea, both TB and CVH are major public health concerns. The number of new onset TB patients is about 40,000 per year in Korea and is continuing to increase [21]. The prevalence of HBV in Korean population is 3.7 % [22], and 0.78 % of the Korean population has an HCV infection [23]. The aim of present study was investigate the incidence and risk factors of DILI in patients with CVH and to compare them to patients without CVH.
Materials and Methods
Study populations
We retrospectively enrolled a total of 128 patients with CVH who were consecutively diagnosed with pulmonary or extrapulmonary TB and receiving standard anti-TB drugs at the Gyeongsang National University Hospital, a tertiary hospital in Korea, from January 2005 to February 2014. Among these, 83 patients were positive for HBV surface antigen (HBsAg) and negative for the HCV antibody (HBV group), 41 were negative for HBsAg and positive for the HCV antibody (HCV group), and 4 were positive for both HBsAg and HCV antibody (HBV + HCV group). The following data were collected from electronic medical records by computer-assisted chart review; age, sex, alcohol ingestion, body mass index (BMI), previous TB history, TB infection site (lung or other), date of anti-TB drugs prescription, regimen of anti-TB drugs, HBsAg, HCV antibodies, HBV DNA, HCV RNA, serial liver function test once in 2 weeks, including aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin, symptoms of hepatitis including anorexia, nausea, vomiting, generalized weakness, abdominal discomfort, and jaundice, and comorbidities including liver cirrhosis, chronic kidney disease, diabetes mellitus, hepatocecullar carcinoma, and other malignancies.
For the purposes of comparison, 251 consecutively patients diagnosed with pulmonary or extrapulmonary TB with negative HBsAg and HCV antibody from January 2013 to February 2014 were enrolled and their respective electronic medical records were analyzed as the control group. If a patient had liver function impairment, the time until onset was measured in days. The mean onset time and standard deviation were calculated. The incidence of DILI was investigated according to patients with and without viral hepatitis. Follow up duration was measured by 12 months in cases without hepatotoxicity. Patients with initial AST or ALT over 2 times the upper limit of normal, initial total bilirubin over 1.5 times the upper limit of normal, less than 3 months of treatment duration, and liver function abnormality caused by a source other than anti-TB drugs were excluded. There were no HIV-infected patients among the enrolled patients. The present study was approved by the Institutional Review Board of the Gyeongsang National University Hospital.
Definitions
The liver function impairment was classified as transient liver function impairment (TLI) and DILI. The definition of TLI and DILI was based on previous studies and literature [1, 16–18, 24]. TLI was defined as AST/ALT levels above the upper limit of normal (40 IU/L), but were still less than three times the upper limit of normal (120 IU/L) and resolved spontaneously, despite continued medication. DILI was defined as liver transaminase levels were exceeded 120 IU/L with symptoms of hepatitis or exceeded 200 IU/L without symptoms. If AST/ALT levels were under 200 IU/L, the case was defined as mild DILI. AST/ALT levels of 200 to 500 IU/L indicated moderate DILI, and AST/ALT levels exceeding 500 IU/L were considered to indicate severe DILI. A baseline liver function test (LFT) abnormality was defined as AST or ALT over 40 IU/L. Alcohol consumption was defined as an intake of more than 30 g/day of alcohol for males and 20 g/day for females [25].
Anti-tuberculosis treatment
In South Korea, treatment of TB is based on the National Tuberculosis Guidelines [26]. They are nearly identical to American and World Health Organization (WHO) guidelines [1, 27]. The recommended treatment is a 6 month regimen consisting of 2 months of INH, RFP, EMB, and PZA, followed by 4 months of INH and RFP. Most patients received daily drugs including INH (300 mg), RFP (450 ~ 600 mg), EMB (800 ~ 1200 mg), and PZA (1,500 mg). After patients develop DILI, additional modes of anti-TB management are used. Patients with DILI are managed in one of two ways based on the physician’s judgment and treatment guidelines [26]: (1) cease the anti-TB treatment and restart treatment when liver transaminase levels fall to less than two times the upper limit of normal, or (2) cease the anti-TB treatment and restart the alternative treatment with non-hepatotoxic drugs or cease the anti-TB treatment and do not restart treatment.
Statistical analysis
SPSS (version 21.0; IBM SPSS statistics) was used for statistical analysis. Continuous variables were compared using the Mann–Whitney U tests. Categorical variables were compared using Fisher’s exact test and the chi-square test. The cumulative incidences of the control, HBV, HCV, and HBV + HCV groups were analyzed using Kaplan-Meier curve and comparison of the differences of incidence was performed using the log-rank test. The association between DILI and the presence of HBV, HCV, CVH, or total patients was evaluated by Cox regression analysis. The risk was expressed by calculating the hazards ratio (HR) and 95 % confidential interval (CI). P-values under 0.05 were considered statistically significant.
Results
Patient characteristics
A total of 379 patients were enrolled in this study. Baseline characteristics of each group are presented in Table 1. There were no significant differences in sex, other malignancies, alcohol ingestion, extrapulmonary TB, BMI, or chronic kidney disease between groups. The control group was significant older than the HBV group. The rate of use of PZA was lower in the HBV group. Incidences of hepatocellular carcinoma and liver cirrhosis were higher in the CVH patients. Baseline LFT abnormalities were more common in CVH patients.
Incidence of hepatotoxicity
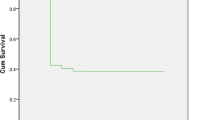
In total patients who received anti-TB treatment, DILI occurred in 13.7 % (52/379). The incidence of total hepatotoxicity (TLI + DILI) was higher in the HBV (34.9 %, p = 0.008), HCV (53.6 %, p = 0.001), and HBV + HCV groups (100 %, p = 0.002) than in the control group (20.7 %). In Table 2, it was shown that the HBV (21.7 %, p = 0.010) and HCV groups (22.0 %, p = 0.040) developed higher TLI than the control group (10.8 %). The incidence of DILI was significantly higher in the HCV (31.7 %, p < 0.001) and HBV + HCV groups (75.0 %, p = 0.002) compared to the control group (10.0 %), but not for the HBV group (13.3 %, p = 0.400). There were no significant differences in the frequencies of severe DILI in patients in the HBV, HCV, HBV + HCV, and control groups. In Kaplan-Meier analysis for the development of DILI, the incidence of DILI in the HCV (p = 0.001) and HBV + HCV groups (p = 0.001) were significantly higher than that of the control group, but not for the HBV group (p = 0.521) (Fig. 1).

Kaplan-Meier curve for occurrence of drug-induced liver injury. The cumulative incidences of drug-induced liver injury in the hepatitis C virus (p = 0.001) and hepatitis B virus + hepatitis C virus groups (p = 0.001) were significantly higher than that of the control group, but not in the hepatitis B virus group (p = 0.521). P-value compared with control group, DILI, drug-induced liver injury; HBV, hepatitis B virus; HCV, hepatitis C virus
Risk factors associated with drug-induced liver injury
In Table 3, we analyzed the risk factors of DILI in the subject population with anti-TB treatment by Cox regression analysis. In univariate analysis, HCV infection, HBV + HCV co-infection, age, HCC, and baseline LFT abnormality were significant factors for DILI. In multivariate analysis, HCV infection (HR = 2.623, 95 % CI: 1.289-5.338, p = 0.008), HBV + HCV co-infection (HR = 9.401, 95 % CI = 2.691-32.841, p < 0.001), age (HR = 1.034, 95 % CI = 1.013-1.054, p = 0.001), and baseline liver function abnormality (HR = 2.331, 95 % CI = 1.238-4.390, p = 0.009) were independent risk factors for DILI.
We performed subgroup analysis to identify risk factors in each viral hepatitis group. In CVH patients, age (HR = 1.039, 95 % CI = 1.009-1.070, p = 0.011) and baseline LFT abnormality (HR = 4.601, 95 % CI = 2.017-10.496, p ≤ 0.001) were independent risk factors for the development of DILI (Table 4). In the HBV group, baseline LFT abnormality (HR = 8.643, 95 % CI = 1.598-46.748, p = 0.012), diabetes (HR = 8.819, 95 % CI = 1.228-63.352, p = 0.030), and HBV DNA ≥ 2000 IU/ml (HR = 5.140, 95 % CI = 1.150-22.978, p = 0.032) were predictors for the development of DILI. In the HCV group, age (HR = 1.091, 95 % CI = 1.014-1.173, p = 0.019) and baseline LFT abnormality (HR = 14.889, 95 % CI = 1.709-129.748, p = 0.014) were significant risk factors of DILI, but detection of HCV RNA was not a significant risk factor. High HBV DNA level (≥2,000 IU/ml) was an independent risk factor for DILI in the HBV group. HCV RNA PCR and HCV genotype were checked in only some of the patients (n = 29 and n = 14). However, the detection of HCV RNA was not significant factor for DILI in the HCV group.
Onset time of drug-induced hepatitis, modes of management and recovery time
There was no significant difference in mean onset time of DILI in patients with and without CVH (83.3 ± 77 days and 43.9 ± 41 days, p = 0.056). Among the 52 patients who developed DILI, 9/25 (36.0 %) of the control group and 3/27 (11.1 %) of CVH patients developed DILI within 2 weeks, which was statistically significant (p = 0.033, data not shown). There was no statistical significance between modes of management after the development of DILI between the control and CVH groups. Among 52 patients with DILI, 12/25 (48 %) and 11/27 (40.7 %) of patients successfully completed treatment with first-line drugs in the groups with and without CVH, respectively (p = 0.509, data not shown). The recovery time after the onset of DILI was longer in the HBV group than the control group, but not in the HCV and HBV + HCV co-infection group (Fig. 2).

Kaplan-Meier curve for recovery from drug-induced liver injury. The recovery rate of drug-induced liver injury in hepatitis B virus (p = 0.040) was significantly higher in the early period than that of the control group, but not in the hepatitis C virus (p = 0.036) and hepatitis B virus + hepatitis C virus groups (p = 0.381). P-value compared with control group. DILI, drug-induced liver injury; HBV, hepatitis B virus; HCV, hepatitis C virus
Discussion
In this study, DILI occurred in 13.7 % of total patients who received anti-TB treatment. It was found that HCV infection and HBV + HCV co-infection were independent risk factors for DILI. However, HBV infection was not a risk factor for DILI. The incidence of DILI was similar in patients with HBV infections without the presence of viral hepatitis. However, TLI was significantly higher in HBV-infected patients than in patients without viral hepatitis.
In previous studies [14, 16, 17], the incidence of DILI in HBV-infected patients was 7 % to 12 %. The incidence of DILI in HCV-infected patients was 9 % to 30 % [12–14, 16, 18]. In our study, the incidence of anti-TB DILI in the control group was 10.0 %. In CVH patients, the incidence of DILI was 13.3 %, 31.7 %, and 75.0 % in the HBV, HCV, and HBV + HCV groups, respectively. Compared to the control group, the incidence of DILI was significantly higher in the HCV and HBV + HCV groups, but not in the HBV group. However, when considering TLI in addition to DILI, the incidence was also statistically significant in the HBV group. There were 4 patients in our subject population that had both HBV and HCV infection. In this group, one patient showed TLI, while the remaining three developed DILI.
In some previous studies, it has been documented that HBV infections increase the risk for DILI. In Hong Kong, Wong et al. found that HBV infections were a significant risk factor for liver dysfunction. However, that study did not classified TLI and DILI, and only defined liver dysfunction as an increase in ALT levels to 1.5 times above the UNL [11]. If we applied that definition to our study, we would find a similar result: a significant incidence of any liver function impairment. In previous studies applied same definition of DILI [14, 16], the incidence of DILI in HBV patients were not significantly increased compared to normal control groups. In the HBV group, high HBV DNA level (≥2,000 IU/ml) is an independent risk factor for DILI (HR = 5.140, Table 4). In a previous study [28], it was recommended that using an antiviral agent to decrease the viral load to prevent the development of liver dysfunction. In the present study, among the 83 patients in HBV group, 16 patients were medicated with an antiviral agent, while 67 patients were not. The administration of an antiviral agent did not decrease the risk of DILI (data not shown).
In the HCV group, there was no statistical significance regarding the detection of HCV RNA, an HCV genotype. A previous study in Taiwan [24], found that a high initial HBV/HCV viral load was a significant risk factor for DILI. In another study, the detection of HCV viral load and HCV genotype were not significant predictors of DILI [12]. The mechanism accounting for the higher incidence of DILI in the HCV group than in the HBV group is not known yet. In a previous study, Wedemeyer et al. showed HCV core protein alters lipid metabolism, contributing to the development of hepatic steatosis. Hepatic steatosis may trigger hepatocyte apoptosis, which facilitates inflammation and fibrosis [29]. Other studies have explained that a high baseline viral load more frequently leads to the development of DILI [24]. A pro-inflammatory environment induced by actively replicating the hepatitis virus may alter the detoxication process and increase drug toxicity [30]. Although, we did not find any associations with BMI and hepatotoxcity, there are some studies indicating low BMI as a risk factor [31]. Further study is needed about the interaction of CVH and high incidence of DILI.
Previous studies have reported that DILI usually occurs within 2 months of the anti-TB treatment [32]. Liu et al. reported that TLI occurred later in CVH patients, but not for DILI [16]. In present study, DILI was more common in the CVH group than the control group after 2 weeks of treatment. In addition, there was no difference in the modes of treatment management of DILI between the control and CVH groups. In previous studies [16–18], the severity of DILI was not significantly different in the control and CVH groups. In another previous study [14], both the HBV and HCV groups had longer durations of AST/ALT elevation compared to the control group. In this study, the recovery time after the onset of DILI was longer in the HBV group than in the control group, but not in the HCV and HBV + HCV co-infection groups.
This study has some limitations. First, because of its retrospective nature, the study may provide inaccurate information about alcohol intake or herbal medication. Second, there was a lack of information about the hepatitis virus in CVH patients, HBV DNA and HCV RNA viral load, HCV genotype, etc. Third, this was a single-center study with a relatively small sample size, especially HBV + HCV co-infection group. Forth, there were so many baseline differences between the 2 main patient groups and the control group such that outcomes would be predicted to be different on this basis alone. Further prospective study with more patients is needed to gleam more detailed information about the hepatitis virus.
Conclusion
HCV infection and HBV + HCV co-infection were associated with anti-TB treatment-induced hepatotoxicity. HBV infection was only associated with TLI. In the total patient population receiving anti-TB treatment, the independent risk factors for DILI were HCV with or without HBV infection, age, and baseline liver function abnormality. It is recommended to carefully monitor for DILI in patients with HCV or HBV + HCV co-infections, old age, and abnormal baseline LFTs.
Abbreviations
- TB:
-
Tuberculosis
- TLI:
-
Transient liver function impairment, DIH, drug induced hepatitis
- HBV:
-
Hepatitis B virus
- HCV:
-
Hepatitis C virus
- LFT:
-
Liver function test
- BMI:
-
Body mass index
- HR:
-
Hazards ratio
- CI:
-
Confidence interval
- CVH:
-
Chronic viral hepatitis
References
Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, et al. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003;167(4):603–62.
Sharifzadeh M, Rasoulinejad M, Valipour F, Nouraie M, Vaziri S. Evaluation of patient-related factors associated with causality, preventability, predictability and severity of hepatotoxicity during antituberculosis [correction of antituberclosis] treatment. Pharmacol Res. 2005;51(4):353–8.
Sharma SK, Balamurugan A, Saha PK, Pandey RM, Mehra NK. Evaluation of clinical and immunogenetic risk factors for the development of hepatotoxicity during antituberculosis treatment. Am J Respir Crit Care Med. 2002;166(7):916–9.
van Hest R, Baars H, Kik S, van Gerven P, Trompenaars MC, Kalisvaart N, et al. Hepatotoxicity of rifampin-pyrazinamide and isoniazid preventive therapy and tuberculosis treatment. Clin Infect Dis. 2004;39(4):488–96.
Tost JR, Vidal R, Cayla J, Diaz-Cabanela D, Jimenez A, Broquetas JM, et al. Severe hepatotoxicity due to anti-tuberculosis drugs in Spain. Int J Tuberc Lung Dis. 2005;9(5):534–40.
Singanayagam A, Sridhar S, Dhariwal J, Abdel-Aziz D, Munro K, Connell DW, et al. A comparison between two strategies for monitoring hepatic function during antituberculous therapy. Am J Respir Crit Care Med. 2012;185(6):653–9.
Saukkonen JJ, Cohn DL, Jasmer RM, Schenker S, Jereb JA, Nolan CM, et al. An official ATS statement: hepatotoxicity of antituberculosis therapy. Am J Respir Crit Care Med. 2006;174(8):935–52.
Dossing M, Wilcke JT, Askgaard DS, Nybo B. Liver injury during antituberculosis treatment: an 11-year study. Tuber Lung Dis. 1996;77(4):335–40.
Pande JN, Singh SP, Khilnani GC, Khilnani S, Tandon RK. Risk factors for hepatotoxicity from antituberculosis drugs: a case–control study. Thorax. 1996;51(2):132–6.
Fernandez-Villar A, Sopena B, Fernandez-Villar J, Vazquez-Gallardo R, Ulloa F, Leiro V, et al. The influence of risk factors on the severity of anti-tuberculosis drug-induced hepatotoxicity. Int J Tuberc Lung Dis. 2004;8(12):1499–505.
Wong WM, Wu PC, Yuen MF, Cheng CC, Yew WW, Wong PC, et al. Antituberculosis Drug-Related Liver Dysfunction in Chronic Hepatitis B Infection. Hepatology. 2000;31:201–6.
Lomtadze N, Kupreishvili L, Salakaia A, Vashakidze S, Sharvadze L, Kempker RR, et al. Hepatitis C virus co-infection increases the risk of anti-tuberculosis drug-induced hepatotoxicity among patients with pulmonary tuberculosis. PLoS One. 2013;8(12):e83892.
Ungo JR, Jones D, Ashkin D, Hollender ES, Bernstein D, Albanese AP, et al. Antituberculosis drug-induced hepatotoxicity. The role of hepatitis C virus and the human immunodeficiency virus. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1871–6.
Devarbhavi H, Singh R, Patil M, Sheth K, Adarsh CK, Balaraju G. Outcome and determinants of mortality in 269 patients with combination anti-tuberculosis drug-induced liver injury. J Gastroenterol Hepatol. 2013;28(1):161–7.
Fernandez-Villar A, Sopena B, Garcia J, Gimena B, Ulloa F, Botana M, et al. Hepatitis C virus RNA in serum as a risk factor for isoniazid hepatotoxicity. Infection. 2007;35(4):295–7.
Liu YM, Cheng YJ, Li YL, Liu CE, Hsu WH. Antituberculosis treatment and hepatotoxicity in patients with chronic viral hepatitis. Lung. 2014;192(1):205–10.
Lee B-H, Koh W-J, Choi M-S, Suh G-Y, Chung M-P, Kim H-j, et al. Inactive HBsAg carrier state and hepatotoxicity during antiTB chemotherapy. Chest. 2005;127(4):1304–11.
Kwon YS, Koh WJ, Suh GY, Chung MP, Kim H, Kwon OJ. Hepatitis C virus infection and hepatotoxicity during antituberculosis chemotherapy. Chest. 2007;131(3):803–8.
S-J HWANG, J-C WU, C-N LEE, F-S YEN, C-L LU, T-P LIN, et al. A prospective clinical study of isoniazid-rifampicin-pyrazinamideinduced liver injury in an area endemic for hepatitis B. J Gastroenterol Hepatol. 1997;12:87–91.
de Castro L, Do Brasil PE, Monteiro TP, Rolla VC. Can hepatitis B virus infection predict tuberculosis treatment liver toxicity? Development of a preliminary prediction rule. Int J Tuberc Lung Dis. 2010;14(3):332–40.
Un-yeoung G, Hyun-jin S, Yeon-kyeng L, Hyosoon Y, Yoon-sung P, Hae-young K, et al. Annual report on the notified tuberculosis in korea. In: Prevention KCfDC, editor. Korea Centers for Disease Control & Prevention: YANG Byung-guk. 2012. p. 12.
Park NH, Chung YH, Lee HS. Impacts of vaccination on hepatitis B viral infections in Korea over a 25-year period. Intervirology. 2010;53(1):20–8.
The Korean Association for the Study of the L. KASL clinical practice guidelines: Management of Hepatitis C. Clin Mol Hepatol. 2014;20(2):89–136.
Wang CW, Lin HY, Shin SJ, Yu ML, Lin ZY, Dai CY, et al. The PNPLA3 I148M polymorphism is associated with insulin resistance and nonalcoholic fatty liver disease in a normoglycaemic population. Liver Int. 2011;31(9):1326–31.
Tarantino G, Saldalamacchia G, Conca P, Arena A. Non-alcoholic fatty liver disease: further expression of the metabolic syndrome. J Gastroenterol Hepatol. 2007;22(3):293–303.
Moon H, Lee J. Korean Guidelines for Tuberculosis. Korea: Joint Committee for the Development of Korean Guidelines for Tuberculosis; 2011.
WHO: Treatment of tuberculosis guidelines, 4th ed. Geneva, World Health Organization, 2010 (WHO/HTM/STB/2009.420). Available: http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf.
Dhiman RK, Saraswat VA, Rajekar H, Reddy C, Chawla YK. A Guide to the Management of Tuberculosis in Patients with Chronic Liver Disease. J Clin Exp Hepatol. 2012;2(3):260–70.
Wedemeyer I, Bechmann LP, Odenthal M, Jochum C, Marquitan G, Drebber U, et al. Adiponectin inhibits steatotic CD95/Fas up-regulation by hepatocytes: therapeutic implications for hepatitis C. J Hepatol. 2009;50(1):140–9.
Schenker S, Martin RR, Hoyumpa AM. Antecedent liver disease and drug toxicity. J Hepatol. 1999;31(6):1098–105.
Tostmann A, Boeree MJ, Aarnoutse RE, de Lange WC, van der Ven AJ, Dekhuijzen R. Antituberculosis drug-induced hepatotoxicity: concise up-to-date review. J Gastroenterol Hepatol. 2008;23(2):192–202.
Sun H-Y, Chen I-L, Gau C-S, Chang S-C, Luh K-T. A Prospective Study of Hepatitis During Antituberculous Treatment in Taiwanese Patients and a Review of the Literature. J Formos Med Assoc. 2009;108(2):102–11.
Acknowledgments
We are grateful to the devoted our collaborators and research coordinators (Jeong Mi Lee, Hye Won Oh, and Ra Ri Cha)
Financial support
There was no financial support in this study
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interests
Author's contributions
WSK and SSL participated in the study design and concept, performed the statistical analysis and participated in data interpretation, and participated in manuscript writing. CML, HongJK, and CYH participated in data collection. HyunJK and THK performed the statistical analysis and participated in data interpretation. WTJ, OJL, and HCC participated in the study design and concept. JWH and HSY participated in data collection and performed the statistical analysis and participated in data interpretation. All authors read and appproved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kim, W.S., Lee, S.S., Lee, C.M. et al. Hepatitis C and not Hepatitis B virus is a risk factor for anti-tuberculosis drug induced liver injury. BMC Infect Dis 16, 50 (2016). https://doi.org/10.1186/s12879-016-1344-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-016-1344-2