

Abstract
Health at birth is an important predictor of long-term outcomes, including education, income, and disability. Recent evidence suggests that maternal disadvantage leads to worse health at birth through poor health behaviors; exposure to harmful environmental factors; worse access to medical care, including family planning; and worse underlying maternal health. With increasing inequality, those at the bottom of the distribution now face relatively worse economic conditions, but newborn health among the most disadvantaged has actually improved. The most likely explanation is increasing knowledge about determinants of infant health and how to protect it along with public policies that put this knowledge into practice.
Income inequality in many developed countries has been rising steadily since the late 1970s, with the United States having recently earned the distinction of being the most unequal of all developed countries (1). In addition to affecting the current generation, rising inequality may have long-term consequences, affecting the distribution of health, human capital, and income of the next generation. This conclusion is based on evidence about the importance of maternal conditions in determining the health and human capital of their offspring, which in turn affects their future economic status. One important way in which maternal circumstances matter is by affecting health at birth, which is an important predictor of long-term outcomes.
We review existing research on the pathways through which conditions associated with maternal economic disadvantage during the prenatal period affect health at birth and children’s outcomes. It is difficult to distinguish between the effects of prenatal conditions and those of genetic inheritance or postnatal “investments” in children. However, mounting evidence suggests that maternal impoverishment during the prenatal period does have a substantial causal impact on infant health, which in turn affects long-term outcomes. Most of this research is based not on randomized controlled trials, which are typically infeasible and/or unethical in this context, but rather on studies of “natural experiments” or on sibling comparisons.
These designs, when well executed, can allow researchers to draw more credible causal inferences than can studies that document simple correlations. For example, although we do not believe genes to be an empirically important cause of inequality, it is theoretically possible that unfavorable genetic inheritance could cause both low maternal income and poor infant health. In such an example, improving income would not improve infant health because both would be driven by an omitted third factor (genes). Natural experiments are events that researchers exploit in an attempt to eliminate confounding due to unobserved or unmeasured variables through a design that mimics the random assignment of controlled experiments. Early studies examining reductions in pollution due to plant closings or recessions provide an important example (2, 3). When an industrial plant closes for economic reasons, there may be a sudden reduction in pollution. As long as the composition of mothers living near the plant does not change too rapidly with the closure, a before and after comparison of women living near the plant and women living further away from the plant can be used to assess the effect of the change in pollution on infant health.
Sibling comparisons control for constant characteristics of the parents (such as genetic inheritance) and hence eliminate this potential source of confounding. For example, to estimate the impact of birth weight (the most common measure of newborn health) on the future outcomes of offspring, one cannot simply compare outcomes of low-birth-weight and normal-birth-weight children because these differences may reflect factors such as genetic inheritance or differential patterns of prenatal investment. If the researcher cannot control for these differences, they will bias the estimated effects of birth weight. Hence, to address the problem of confounding, researchers have used twinning as a natural experiment (4–7). Twins typically differ in their birth weight because of location in the uterus and/or differences in the placentas (a “natural” source of random variation), but their genetic inheritance and postnatal environments are very similar. As a result, comparing the long-term outcomes of twins born with different birth weights allows one to estimate the causal impact of birth weight on outcomes controlling for these two important confounders. Such studies, which are typically based on large national samples, have shown that children of lower birth weight have substantially worse adult outcomes than those of their own twins or closely spaced siblings in terms of schooling attainment, test scores, employment, use of disability programs, wages, and adult health (4–7).
This Review describes research, largely based on sibling comparisons or natural experiments, on the ways in which maternal conditions during the prenatal period affect newborn health and later offspring outcomes. Specifically, the focus is on the following four domains of maternal disadvantage: (i) poor health behaviors during the prenatal period (more smoking, overweight, and neglect of prenatal care); (ii) greater exposure to harmful environmental factors, including the direct effect of toxic pollutants, violence, and stress, combined with a lower likelihood of taking action to avoid potential harms; (iii) poorer access to medical care, including contraception, leading to a greater likelihood of unplanned pregnancy; and (iv) worse underlying health, including poorer nutrition. We will show that all of these factors are associated with worse infant health and with poorer future outcomes, although there are policies that have been shown to be effective in breaking the cycle.
Prenatal Conditions and Offspring Outcomes
The Relationship Between Maternal Disadvantage and Health at Birth
Figure 1 illustrates the huge inequality in health at birth as proxied by the incidence of low birth weight, that exists even in a rich country such as the United States (low birth weight, a common measure of health at birth, is defined as birth weight less than 2500 g) (8). Because U.S. natality data do not include maternal income, we rely on other measured characteristics that are strongly related to income—namely, maternal race, marital status, and education. African American, single, and less educated mothers are all (independently) more likely to be economically disadvantaged. Moreover, all three groups are more likely to have a low-birth-weight baby, as shown in Fig. 1. In the absence of information on income, we use these three characteristics to proxy for maternal advantage, defining the most economically advantaged as non-Hispanic white, married, college-educated mothers and the most economically disadvantaged as African American, unmarried, and less than a high school education. Using census data from the American Community Survey, we calculated that the average household income for women 18 to 40 years old with at least one child less than 5 years old in 2010 to 2012 was $120,655 for the “advantaged” group, whereas the corresponding figure for the “disadvantaged” group was $16,497, suggesting that our proxies for economic advantage are reasonable. The last pair of bars in Fig. 1 show that the incidence of low birth weight among the most disadvantaged is more than three times that of the most advantaged mothers (9).
Fig. 1. Differences in the percent of U.S. infants with birth weight <2500 g, by maternal characteristics, 2011.

Data was calculated by using singleton births to mothers age 19 to 39 years from the U.S. National Individual-Level Natality Data (birth records). The following states are excluded because education is inconsistently coded over time: Alabama, Alaska, Arizona, Arkansas, Connecticut, Hawaii, Maine, Massachusetts, Minnesota, Mississippi, New Jersey, Rhode Island, Virginia, and West Virginia. We focus on singleton births because multiple births are much more likely to be low birth weight, and many multiple births result from assisted reproductive technology. Sample sizes are printed over each bar. Given the large sample sizes, SEMs are very small (<0.15 percentage points).
The difference between the most and least advantaged mothers has declined over the past 20 years (Fig. 2), suggesting that birth weight is indeed malleable and influenced by many factors (10). It is remarkable that health at birth continued to improve in the face of growing income inequality over the same period (11). How did conditions improve for babies, when they were deteriorating for many of their mothers? Our discussion will shed light on policies that may have helped to counteract the effects of growing income inequality.
Fig. 2. Trends in percent low birth weight by maternal socioeconomic status (SES).

The sample is defined as in Fig. 1. Disadvantaged is defined as African American, less than a high school education, and unmarried. Advantaged is defined as white, college education, and married.
Explaining the Maternal Socioeconomic Status and Offspring Outcomes Relationship
The studies surveyed in this section all rely on natural experiments or sibling comparisons to estimate causal effects. They fall into two groups. The first consists of studies of the impact of prenatal conditions on newborn health (usually measured with birth weight). These studies do not show a direct connection between maternal prenatal conditions and later offspring outcomes but instead rely on existing studies that have established a strong relationship between newborn health and long-term outcomes, including intelligence quotient (IQ), education, employment, and income. The second group of studies link prenatal maternal conditions directly with long-term offspring outcomes.
Maternal Behavior
It is perhaps unsurprising that consumption of tobacco, alcohol, and illegal drugs during pregnancy is associated with adverse birth outcomes, or that good nutrition and better access to medical care are associated with positive outcomes. Health behaviors during pregnancy are typically better among more economically advantaged women (12). For example, in the United States in 2011 18% of the most disadvantaged women smoked during pregnancy compared with 1% of the most advantaged women (Fig. 3). There are a number of randomized controlled trials of smoking cessation interventions among pregnant women that link reductions in smoking during pregnancy with improved birth outcomes such as prematurity and birth weight. These studies have been reviewed elsewhere (13).
Fig. 3. Differences in maternal health and behavior by maternal SES, United States 2011.
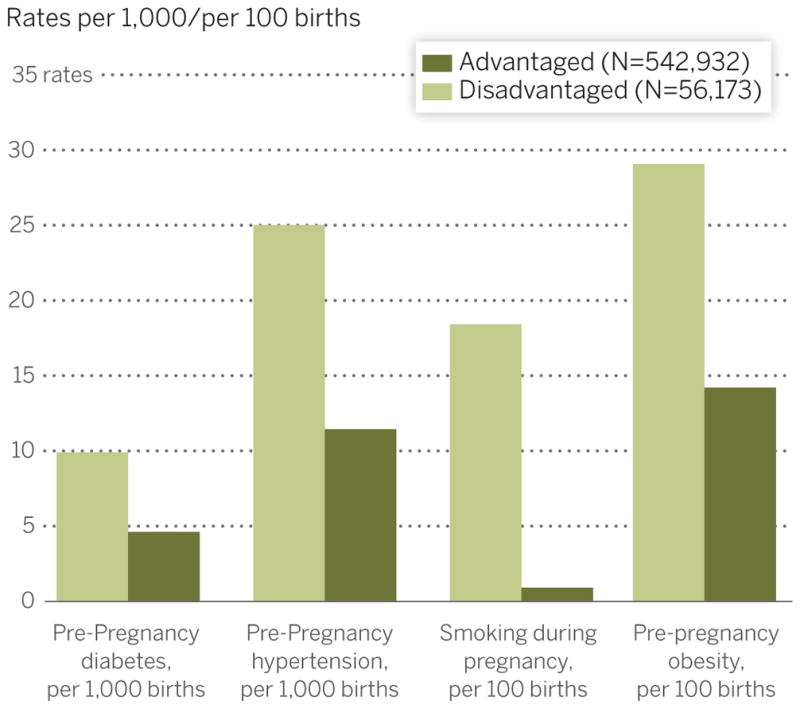
The sample is defined as in Fig. 1. Disadvantaged is defined as African American, less than a high school education, and unmarried. Advantaged is defined as white, college education, and married. Given the large sample sizes, SEMs are very small (<0.2 units).
Other studies based on natural experiments or sibling comparisons have also found that smoking has a negative impact on newborn health and that this does not simply reflect other adverse circumstances affecting mothers who happen to smoke (14–16). For example, researchers using data from 1.5 million births in New Jersey between 1989 and 2003 compared the birth weights of sibling pairs in which the mother smoked during one pregnancy but not the other. They estimated that conditional on any smoking, smoking at the mean number of cigarettes smoked per day (10) increases the probability of low birth weight by 1.8 percentage points on a baseline of 8.9% low birth weight in their sample (15).
Environmental Factors: Pollution, Violence, and Stress
Another way in which maternal economic status influences newborn health is through exposure to harmful environmental factors such as pollution, violence, and stress. There is growing evidence that even relatively low levels of pollution have negative effects on infant health. Several recent studies consider variation in pollution owing to policy changes as a “natural experiment” that can help to identify the effect of in utero exposure to pollution on birth weight, as well as on later outcomes such as child test scores and adult earnings (17–19). For example, the introduction of electronic toll-collection devices (E-ZPass) in New Jersey and Pennsylvania greatly reduced auto emissions in the vicinity of toll plazas and reduced the incidence of low birth weight by about one percentage point in the 2 km surrounding the toll plaza (17).
Because of lower housing costs, poor women are more likely to live near, and therefore to be exposed to, sources of pollution. A study of all births in five large U.S. states found that African American women and less-educated women (two correlates of economic disadvantage) are more likely to live within 200 m of Superfund hazardous waste sites or factories emitting toxic releases and that this pattern holds even within small areas defined by ZIP codes (20). Moreover, less-educated and minority women are less likely to move to cleaner areas between births. When Superfund sites are cleaned up, the population living in the area immediately surrounding the site becomes more economically advantaged (again as proxied by race and education). Similarly, a study of all births in New Jersey over a 10-year period found that less-educated women were less likely to move away from water districts with drinking-water quality violations between births (21).
Poor women and minority women are also more likely to be the victims of violence, especially intimate partner violence (IPV). More specifically, African American and Hispanic women are twice as likely to be the victims of IPV than are white women, and women with incomes less than $25,000 per year are two and half times as likely to be victimized than are those with incomes greater than $25,000 (22).
Changes in local, county-level policing policies have been effective in reducing IPV, and research has used the rollout of these policies to estimate the impact of IPV on birth outcomes (23). These policy changes involve reductions in police and prosecutorial discretion as well as increasing the availability of community resources for victims (24). Reductions in levels of violence resulting from these policies have been used to show that hospitalization for an assault while pregnant reduces birth weight by 163 g, on average. Thus, although these policies _target women, they have substantial positive effects on newborn health and well-being, as well (23).
In addition to the direct negative effect of violence on maternal and child health, violence may also indirectly harm pregnant women by increasing their exposure to stress. Although stress is difficult to measure and may have different effects depending on whether it is chronic or episodic, greater exposure to stress among the poor and disadvantaged has been linked with worse physical and mental health. Research in neurobiology has identified abnormal levels and fluctuations in cortisol (often referred to as the “stress hormone”) and the dysregulation of the hypothalamic-pituitary-adrenal axis as the primary underlying mechanism (25, 26). More recently, given that cortisol crosses the placenta, researchers have focused on the negative effects of exposure to stress in utero on offspring outcomes. Comparisons of siblings show that those who were exposed to high levels of the stress hormone cortisol in utero have lower IQ levels at age 7 and complete 1 fewer year of schooling (27).
An innovative study of all births to mothers with Arabic names in California in the 6 months after the 2001 terrorist attacks in the United States found that the incidence of poor birth outcomes was substantially elevated for this group relative to that for non-Arabic–named mothers. The study argues that Arabic-named mothers suffered particularly strong psychological stress in the aftermath of the attacks, which in turn had a negative impact on their babies (28). Children in utero in areas in the path of hurricanes also have worse outcomes than those of unaffected siblings, with the most likely explanation being exposure to maternal stress (29, 30).
Access to Medical Care and Family Planning
Previous work has shown that the Medicaid expansions of the 1980s, which expanded health insurance coverage for pregnant women, reduced the probability of low birth weight (slightly) and infant mortality (more strongly) among low-income women (31–33). More recent work has focused on Medicaid (and other publicly funded) expansions of coverage for family-planning services. Poor women are more likely to have unplanned pregnancies (34) and to space their pregnancies more closely together (35). Both factors are thought to reflect inadequate access to family-planning services, and both have been linked to worse birth outcomes (36–38). Hence, offering poor women access to more comprehensive family-planning technologies may have the potential to improve birth outcomes for poor mothers.
Two recent studies have exploited geographic variation in access to family-planning services in order to estimate their impact on fertility and child outcomes. The first used state-level expansions in Medicaid eligibility for family-planning services to estimate the impact of access to family planning on fertility. The authors found that expanding Medicaid coverage for family planning reduced birth rates among the “near poor” (the poor were already covered) by between 2 and 4% (39). The second study used historical data on the timing of access to oral contraception (which differed greatly by state) and on federal family-planning grants to poor areas in order to estimate the impact of these policies on children’s outcomes. Both types of policies resulted in declines in fertility (40). Although infant health did not improve measurably in areas that received grants to subsidize contraception/family planning, maternal resources available to children did, as did the children’s long-term well-being. Children born in areas and years that had access to subsidized family planning saw substantial improvements in educational attainment and earnings in adulthood (41, 42).
Worse Maternal Health, Including Nutrition
Disadvantaged women are in worse underlying health than are their more advantaged counterparts. For example, in 2011 disadvantaged pregnant women were twice as likely to be obese or to have preexisting conditions of diabetes or hypertension as compared with their advantaged counterparts (Fig. 3). Some of this elevated risk may be due to their own histories of disadvantage. This history of disadvantage is what underlies the “weathering hypothesis,” first proposed by Geronimus to explain the fact that the African American–white gap in infant mortality increases with maternal age (43). Historical U.S. data on mothers born between 1961 and 1990 shows that mothers who were born in a high disease environment (measured by using high post-neonatal mortality rates) were more likely to have diabetes than were other women at the time they delivered their own infants. Moreover, these women were also more likely to have low-birth-weight babies (44, 45).
In addition to being in worse underlying health, disadvantaged women also have greater exposure to and are more susceptible to contagious diseases such as seasonal influenza. Hence, they may be disproportionately affected by pandemics, which can negatively affect fetal development (46). There are a number of factors that can potentially explain disadvantaged women’s greater susceptibility, including the fact that disadvantaged women are more likely to live in crowded homes, are more reliant on public transportation, are less likely to be immunized, are less able to stay home from work when ill, and are less likely to believe the influenza vaccine to be effective (47). They are also more likely to have asthma—a complicating factor—and less likely to have access to health care.
Exposure to influenza in utero has been linked with both worse newborn health and worse long-term outcomes for offspring. Recent research has documented spikes in prematurity among siblings nearing full term in months with greater prevalence of influenza (48). Researchers have also relied on unexpected pandemics to estimate the causal impact of influenza on offspring outcomes (49–51). For example, the influenza epidemic of 1918 affected different parts of the country at different times. A study using decennial census data from the United States to examine the long-term impacts of in utero exposure to the epidemic shows that affected cohorts had lower earnings and educational attainment and higher probabilities of being disabled decades later (49). World War I is a possible confounder because it could have affected the type of women who became pregnant in 1918 (that is, the wives of soldiers may have been less likely to conceive). However, recent research examining the effect of the pandemic in Taiwan (which was not involved in WWI) finds similar effects (52). Moreover, the 1957 flu epidemic in Great Britain had negative effects on birth weight, although only for the children of the least healthy mothers: smokers and women of below-average height, which is a marker for poor nutrition in childhood (51).
Disadvantaged women are also less likely to gain the recommended weight during pregnancy (30% of disadvantaged versus 16% of more advantaged pregnant women gained less than the recommended amount in 2011) (53). A number of randomized controlled trials of nutritional supplementation during pregnancy, mostly in developing countries, have shown that relatively inexpensive nutritional supplements often increase birth weight (54). Other studies examine specific micronutrient deficiencies. For example, a study of periodic iodine supplementation programs in Tanzania found that children from cohorts that benefited from supplementation in utero attain a third to a half of a year more schooling than do siblings who did not benefit (55).
A number of recent studies have examined the short- and long-term effects of nutritional deprivation during pregnancy that occurs as a result of a fasting during Ramadan among Muslims in both developed and developing countries. Because Ramadan moves through the Gregorian calendar, it is possible to separate the effects of the fast from seasonal effects. Pre-natal exposure to Ramadan in early pregnancy is associated with lower birth weight and an increase in the likelihood of disability in adulthood, even in rich countries such as the United States (56).
Birth Weight and Parental Investments
Poor health at birth will only have lasting effects if parents are unable or unwilling to offset its impacts through postnatal parental investments. There are two potential mechanisms at work. First, higher-income parents have more money to invest in their children and so may be better able to offset the effects of poor infant health (57, 58). Second, postnatal investments may be more productive for those born healthier; that is, prenatal and postnatal investments may prove to be complementary (59).
Existing evidence on the latter pathway is based on studies with long-term follow-up and suggests that newborn health and postnatal investments are indeed complementary (60). Perhaps the best example of such a study is the Infant Health and Development Program (IHDP), which randomized low-birth-weight infants to an intensive preschool program and a less intensive control program. The IHDP found significant, positive, and sustained (to age 18 years) effects of the enriched intervention on cognitive test scores, but only in children with birth weights between 2000 and 2500 g (that is, at the higher end of the low-birth-weight distribution). Among children with birth weights below 2000 g, program effects were negligible (61). Similarly, a recent study of children from the National Collaborative Perinatal Project found that a pre-school intervention in a group of disadvantaged children was effective in raising the IQ of infants with the highest cognitive ability in the group but did not raise the IQ of others, although the intervention may still have had positive effects on noncognitive skills (62).
These examples highlight an important caveat to studies of long-term outcomes among low-birth-weight infants, which is that, of necessity, they follow cohorts born many years ago. Medical advances in the treatment of low-birth-weight infants may have increased the efficacy of post-natal interventions among the lightest infants today, relative to what was seen in previous cohorts. At the same time, infants of lower and lower birth weight are surviving, and their long-term prognosis may be worse than that of the lightest infants in earlier cohorts.
Thus, although considerable uncertainty remains, the available evidence suggests that the initial health disadvantages associated with being born to a poor mother are likely to be exacerbated over time: Children with poorer initial health endowments typically receive fewer post-natal investments, and the investments that they do receive may be less effective. This mechanism can potentially explain the considerable persistence of in utero conditions on later offspring outcomes. It can also explain why the long-term impact of low birth weight is greater when children are born into poverty (63).
Given the importance of maternal prenatal conditions in perpetuating inequality across generations, we next consider evidence regarding the effectiveness of public interventions in breaking the cycle of poverty.
Effectiveness of Public Programs in Breaking the Cycle of Poverty
Existing Programs _targeting the Prenatal Period
As discussed above, health insurance, measures to curb domestic violence, and family-planning services have had positive effects on infant health and longer-term outcomes. Food supplementation programs also appear to show consistent benefits, even in rich countries. For example, the Supplemental Feeding Program for Women, Infants, and Children (WIC) was in the 1970s rolled out gradually, which effectively granted access to some mothers before others. For mothers who were high school dropouts and mothers in high-poverty counties, the introduction of WIC in the mother’s county of residence reduced the proportion of low-birth-weight births by ~1% (64). Conversely, the closing of WIC centers has been associated with reductions in pregnancy weight gain and increases in the incidence of low birth weight among mothers with a high school education or less (65).
The Food Stamps program was also rolled out on a county-by-county basis, and its introduction reduced the incidence of low birth weight by 1% among whites and by as much as 1.5% among African Americans (66). A follow-up study examining long-term outcomes found that access to food stamps in early childhood led to a significant reduction in the incidence of “metabolic syndrome” (obesity, high blood pressure, and diabetes) as well as an increase in economic self-sufficiency among women (67).
Another program that has been shown to be effective in terms of improving short- and long-term outcomes is the Nurse Family Partnership (NFP) program, a modified version of which is being expanded through the Affordable Care Act. NFP programs provide nurse home visits to poor, unmarried, young women who are pregnant for the first time. The visits occur monthly during the pregnancy and during the first 2 years of the child’s life. Nurses provide guidance to pregnant women and new mothers regarding healthy behaviors, competent care of children, and personal maternal development. Two randomized controlled trials with long-term follow-up found significant reductions in child abuse and adolescent criminal activity among the children, as well as improvements in the children’s academic achievement. Improvements were greatest among children whose mothers had the lowest levels of intelligence and/or poor mental health (68, 69).
Postnatal Interventions
Although our focus has been on the role of maternal prenatal conditions and newborn health, there is evidence that intervening in the post-natal period can also be effective. In particular, early-education programs and income-transfer programs have been shown to improve long-term child outcomes among low-income families (70, 71). Reviews of the evidence suggest that intervening during the preschool years is more effective than post-school intervention, although many evaluations of interventions later in life suffer from short follow-up periods. Specifically, only programs that start before the age of 3 years seem to have long-lasting effects on IQ. (70) However, intensive, center-based pre-school programs such as the Perry Preschool and Abecederian programs have had large long-term positive effects on children largely because they improved noncognitive or “character” skills rather than through improvements in IQ, which suggests that an exclusive focus on raising IQ may be misguided (72).
Means-tested income transfer programs have also been found to improve maternal health and child outcomes. In particular, researchers in the U.S. (73–75) and Canada (76) have exploited changes in cash transfers to low-income working families in order to measure the impact of income transfers on child outcomes. These studies found improvements in maternal mental health as well as children’s cognitive test scores, which is an important predictor of long-term economic outcomes. However, women become eligible for these particular programs (among others) only once they have given birth. Given the research on the importance of prenatal conditions, such policies are potentially missing a major window of opportunity.
Conclusions: Implications for Policy and Future Research
Over the past several decades, inequality has been increasing in many developed countries, largely because of economic forces described elsewhere in this issue (11, 77). Other things being equal, one would have expected relative health at birth to deteriorate along with economic conditions for those at the bottom of the distribution. However, other things were not equal: Health at birth bucked this trend and improved steadily for the most disadvantaged in both relative and absolute terms, even during the Great Recession. We now know that the fetus is particularly vulnerable to myriad health insults, but we also know much more about how to protect infants from these shocks.
New knowledge about what matters for fetal health suggests many protective factors, including increasing the prevalence of influenza vaccination for pregnant women, which helps to prevent premature delivery and fetal damage; the expansion of programs such as NFP; supplementing the food and nutrition of pregnant mothers through government programs such as WIC and SNAP (the Supplemental Nutrition Assistance Program, formerly Food Stamps); advances in pollution control that have reduced exposures to harmful toxins; new legal structures that have reduced the incidence of violence against women; the growth of income transfer programs for the near poor and nonpoor (although not the poorest families); and a better understanding of the relationship between contraception, birth spacing, and maternal and fetal health.
Although research on the fetal origins of adult health is exciting and promising, some rather basic questions remain. Looking backward, we can ask, how much of the recent gains in fetal health are due to the various specific factors we have discussed? Which public policies and programs have had the most impact in counteracting the negative effects of growing inequality on infant health, and which are most cost-effective? It would be useful to know, for example, how exposure to diseases such as influenza compares with exposure to common environmental toxicants, but the science is not yet sufficiently advanced to allow these comparisons. Looking forward, we can ask, what are the most promising strategies for continuing to improve fetal health, and how much will this improvement reduce inequality in years to come?
Supplementary Material
Acknowledgments
The authors thank H. Schwandt for assistance in preparing the figures. J.C. received financial support from the John D. and Catherine T. MacArthur Foundation and for support from U.S. Environmental Protection Agency (EPA) grant EPA G2009-STAR-B1.
Footnotes
The authors have no conflicts of interest to report.
REFERENCES AND NOTES
- 1.Central Intelligence Agency. The World Factbook 2013–2014. Cental Intelligence Agency; Washington, DC: 2013. [Google Scholar]
- 2.Chay KY, Greenstone M. Q J Econ. 2003;118:1121–1167. [Google Scholar]
- 3.Parker JD, Mendola P, Woodruff TJ. Epidemiology. 2008;19:820–823. doi: 10.1097/EDE.0b013e3181883d5d. [DOI] [PubMed] [Google Scholar]
- 4.Black SE, Devereux PJ, Salvanes KG. Quarter J Econ. 2007;122:409–439. [Google Scholar]
- 5.Oreopoulos P, Stabile M, Roos L, Walld R. J Hum Resour. 2008;43:88–138. [Google Scholar]
- 6.Royer H. Am Econ J Appl Econ. 2009;1:49–85. [Google Scholar]
- 7.Bharadwaj P, Eberhard J, Neilson C. Do initial endowments matter only initially? The persistent effect of birth weight on school achievement health at birth, parental investments, and academic outcomes. Working paper, University of California at San Diego, Economics Working Paper Series (2010-09-16) [Google Scholar]
- 8.If one looks at all births, the fraction of low birth weight among white college-educated mothers has increased more than suggested with Fig. 2 because these mothers are more likely than others to use assisted reproductive technology.
- 9.Although much of the literature focuses on low birth weight as a summary of health at birth, disparities are also present if we look at alternative indicators. Prematurity is examined in fig. S1. Infant mortality for African Americans and whites is shown in fig. S2 over the same time period. Information about the mother’s education and marital status comes from birth records, so infant mortality by education or marital status groups must be constructed by using linked birth and infant death records, which are missing from some years of the data and are only available up to 2006. Figures S3 and S4 are similar to Figs. 2 and 3, except that they include only mothers 20 to 30 years of age. All of these figures suggest that the trends in low birth weight are not anomalous but are present in other measures of infant health.
- 10.More detailed overviews of factors that have been shown to influence birth weight and of policies that have been shown to be effective in ameliorating the long-term consequences of low birth weight are available in (78).
- 11.Piketty T, Saez E. Science. 2014;344:838–843. doi: 10.1126/science.1251936. [DOI] [PubMed] [Google Scholar]
- 12.This is not always the case; for example, higher-income women are more likely to drink during pregnancy, and alcohol is known to have potentially negative effects on the fetus, although this has been difficult to establish in population studies. However, a recent Swedish study links increases in in utero alcohol exposure, because of a temporary relaxation of drinking laws, to lower adult educational attainment, cognitive ability, wages, and employment (79).
- 13.Chamberlain C, et al. Cochrane Database Syst Rev. 2013;10:CD001055. doi: 10.1002/14651858.CD001055.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lien DS, Evans WN. J Hum Resour. 2005;40:373–392. [Google Scholar]
- 15.Currie J, Neidell M, Schmieder JF. J Health Econ. 2009;28:688–703. doi: 10.1016/j.jhealeco.2009.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bharadwaj P, Johnsen JV, Loken KV. Smoking Bans, Maternal Smoking and Birth Outcomes, Institute for the Study of Labor (IZA) Discussion Papers 7006. IZA; Bonn, Germany: 2012. [Google Scholar]
- 17.Currie J, Walker R. Am Econ J Appl Econ. 2011;3:65–90. [Google Scholar]
- 18.Sanders NJ. J Hum Resour. 2012;47:826–850. [Google Scholar]
- 19.Isen A, Rossin-Slater M, Walker WR. Every breath you take—Every dollar you’ll make: The long-term consequences of the Clean Air Act of 1970. Working paper 19858, National Bureau of Economic Research (NBER) 2013 [Google Scholar]
- 20.Currie J. Am Econ Rev. 2011;101:1–22. doi: 10.1257/aer.101.3.435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Currie J, Graff-Zivin JS, Meckel K, Neidell MJ, Schlenker W. Something in the water: Contaminated drinking water and infant health. Working paper 18876, NBER. 2013 doi: 10.1111/caje.12039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Vest JR, Catlin TK, Chen JJ, Brownson RC. Am J Prev Med. 2002;22:156–164. doi: 10.1016/s0749-3797(01)00431-7. [DOI] [PubMed] [Google Scholar]
- 23.Aizer A. J Hum Resour. 2010;46:518–538. doi: 10.1353/jhr.2011.0024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Arguably the single most important policy change was Congressional passage of the National Violence Against Women Act of 1994, which provided $1.6 billion in resources for local law enforcement and community groups.
- 25.McEwen BS, Gianaros PJ. Ann N Y Acad Sci. 2010;1186:190–222. doi: 10.1111/j.1749-6632.2009.05331.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Seeman T, Epel E, Gruenewald T, Karlamangla A, McEwen BS. Ann N Y Acad Sci. 2010;1186:223–239. doi: 10.1111/j.1749-6632.2009.05341.x. [DOI] [PubMed] [Google Scholar]
- 27.Aizer A, Stroud L, Buka S. Working paper 18422, NBER. 2012. Maternal stress and child outcomes: Evidence from siblings. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lauderdale DS. Demography. 2006;43:185–201. doi: 10.1353/dem.2006.0008. [DOI] [PubMed] [Google Scholar]
- 29.Currie J, Rossin-Slater M. J Health Econ. 2013;32:487–503. doi: 10.1016/j.jhealeco.2013.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Currie and Rossin-Slater (29) did not include any direct measures of stress but assumed that mothers in the hurricane’s direct path were subject to greater stress than were mothers in similar areas off the path.
- 31.Currie J, Gruber J. J Polit Econ. 1996;104:1263–1296. [Google Scholar]
- 32.Lin W. Health Econ. 2009;18:823–841. doi: 10.1002/hec.1407. [DOI] [PubMed] [Google Scholar]
- 33.They found that increasing Medicaid eligibility by 30 percentage points reduced the probability of a low-birth-weight birth by 1.9% and infant mortality by 8.5%.
- 34.Finer LB, Zolna MR. Contraception. 2011;84:478–485. doi: 10.1016/j.contraception.2011.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kost K, Forrest JD. Fam Plann Perspect. 1995;27:11–17. [PubMed] [Google Scholar]
- 36.Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. JAMA. 2006;295:1809–1823. doi: 10.1001/jama.295.15.1809. [DOI] [PubMed] [Google Scholar]
- 37.Zhu BP. Int J Gynaecol Obstet. 2005;89:S25–S33. doi: 10.1016/j.ijgo.2004.08.002. [DOI] [PubMed] [Google Scholar]
- 38.Smits LJ, Essed GG. Lancet. 2001;358:2074–2077. doi: 10.1016/S0140-6736(01)07105-7. [DOI] [PubMed] [Google Scholar]
- 39.Kearney MS, Levine PB. Rev Econ Stat. 2009;91:137–151. doi: 10.1162/rest.91.1.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bailey MJ. Working paper 19493, NBER. 2013. Fifty years of family planning: New evidence on the long-run effects of increasing access to contraception. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.These results echo earlier findings that the legalization of abortion in the United States improved the outcomes of surviving cohorts of children (80).
- 42.Evidence that restricting Medicaid funding of abortions increased birth rates is available in (81).
- 43.Geronimus AT. Soc Sci Med. 1996;42:589–597. doi: 10.1016/0277-9536(95)00159-x. [DOI] [PubMed] [Google Scholar]
- 44.Almond D, Currie J, Herrmann M. Labour Econ. 2011;19:475–483. [Google Scholar]
- 45.Similarly, the eradication of malaria in the U.S. South produced gains for the affected cohorts (82). Improvements in health in the late 1800s and early 1900s have been associated with improved health at older ages (83).
- 46.Quinn SC, et al. Am J Public Health. 2011;101:285–293. doi: 10.2105/AJPH.2009.188029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wooten KG, Wortley PM, Singleton JA, Euler GL. J Vaccine. 2012;6:6927–6934. doi: 10.1016/j.vaccine.2012.08.036. [DOI] [PubMed] [Google Scholar]
- 48.Currie J, Schwandt H. Proc Natl Acad Sci USA. 2013;110:12265–12270. doi: 10.1073/pnas.1307582110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Almond D. J Polit Econ. 2006;114:672–712. [Google Scholar]
- 50.Nelson RE. Health Econ. 2010;19:1181–1192. doi: 10.1002/hec.1544. [DOI] [PubMed] [Google Scholar]
- 51.Kelly E. J Hum Resour. 2011;46:669–694. [Google Scholar]
- 52.Lin M-J, Liu E. Working paper. University of Houston; Aug, 2013. Does ‘in utero’ exposure to illness matter? The 1918 influenza epidemic in Taiwan as a natural experiment. [DOI] [PubMed] [Google Scholar]
- 53.The corresponding figures for infants with gestations of 39 to 41 weeks are 0.243 and 0.138, although excessive weight gain during pregnancy is also associated with poor pregnancy outcomes (84). In addition, high weight gain is actually less common in disadvantaged women (85).
- 54.Abu-Saad K, Fraser D. Epidemiol Rev. 2010;32:5–25. doi: 10.1093/epirev/mxq001. [DOI] [PubMed] [Google Scholar]
- 55.Field E, Robles O, Torero M. Am Econ J Appl Econ. 2009;1:140–169. [Google Scholar]
- 56.Almond D, Mazumder B. Am Econ J Appl Econ. 2011;3:56–85. [Google Scholar]
- 57.Guryan J, Hurst E, Kearney M. J Econ Perspect. 2008;22:23–46. [Google Scholar]
- 58.Yeung WJ, Linver MR, Brooks-Gunn J. Child Dev. 2002;73:1861–1879. doi: 10.1111/1467-8624.t01-1-00511. [DOI] [PubMed] [Google Scholar]
- 59.There is a third potential mechanism that has to do with parental preferences. Parents may want to equalize outcomes among their children (in which case, they would invest more in the least healthy); or, they may want to have at least one child who is very successful, in which case they might invest most in the healthiest child. Evidence on this point is somewhat mixed in developed countries (86, 87).
- 60.Cunha F, Heckman J, Schennach S. Econometrica. 2010;78:883–931. doi: 10.3982/ECTA6551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.McCormick MC, et al. Pediatrics. 2006;117:771–780. doi: 10.1542/peds.2005-1316. [DOI] [PubMed] [Google Scholar]
- 62.Aizer A, Cunha F. Working paper 18429, NBER. 2012. The production of human capital: Endowments, investments and fertility. [Google Scholar]
- 63.Currie J, Moretti E. J Labor Econ. 2007;25:231–264. [Google Scholar]
- 64.Hoynes HW, Page ME, Stevens AH. J Econ Perspect. 2009;20:47–68. [Google Scholar]
- 65.Rossin-Slater M. J Public Econ. 2013;102:51–69. doi: 10.1016/j.jpubeco.2013.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hoynes H, Schanzenbach DW, Almond D. Rev Econ Stat. 2011;93:387–403. [Google Scholar]
- 67.Hoynes H, Schanzenbach DW, Almond D. Working paper 18535, NBER. 2012. Long run impacts of childhood access to the safety net. [Google Scholar]
- 68.Eckenrode J, et al. Arch Pediatr Adolesc Med. 2010;164:9–15. doi: 10.1001/archpediatrics.2009.240. [DOI] [PubMed] [Google Scholar]
- 69.Olds DL, et al. Pediatrics. 2007;120:e832–e845. doi: 10.1542/peds.2006-2111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Heckman J, Pinto R, Savelyev P. Am Econ Rev. 2013;103:2052–2086. doi: 10.1257/aer.103.6.2052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Campbell F, et al. Science. 2014;343:1478–1485. doi: 10.1126/science.1248429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Heckman J, Kautz T. Working paper 19656, NBER. 2013. Fostering and Measuring Skills: Interventions that Improve Character and Cognition. [Google Scholar]
- 73.Dahl G, Lochner L. Am Econ Rev. 2012;102:1927–1956. [Google Scholar]
- 74.Evans W, Garthwaite C. Working paper 18206, NBER. 2011. Giving Mom a break: The effect of higher EITC payments on maternal health. [Google Scholar]
- 75.Hoynes H, Miller D, Simon D. Income, the Earned Income Tax Credit, and infant health. Working paper 18206 NBER. 2012 [Google Scholar]
- 76.Milligan K, Stabile M. Am Econ J Econ Pol. 2011;3:175–205. [Google Scholar]
- 77.Autor DH. Science. 2014;344:843–851. doi: 10.1126/science.1251868. [DOI] [PubMed] [Google Scholar]
- 78.Almond D, Currie J. In: Handbook of Labor Economics. Card D, Ashenfelter O, editors. Elsevier; Amsterdam: 2011. pp. 1315–1486. [Google Scholar]
- 79.Nilsson JP. Working paper. Institute for International Economic Studies; 2014. Alcohol Availability, Prenatal Conditions, and Long-term Economic Outcomes. available at https://sites.google.com/site/nilssonjanpeter. [Google Scholar]
- 80.Ananat E, Gruber J, Levine P, Staiger D. Rev Econ Stat. 2009;91:124–136. [Google Scholar]
- 81.Bitler MP, Zavodny M. Soc Sci Med. 2010;5:918–924. doi: 10.1016/j.socscimed.2010.05.046. [DOI] [PubMed] [Google Scholar]
- 82.Bleakley H. Am Econ J. 2010;2:1–45. doi: 10.1257/app.2.1.165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Ferrie J, Rolf K. Explor Econ Hist. 2011;48:445–460. [Google Scholar]
- 84.Ludwig DS, Currie J. Lancet. 2010;376:984–990. doi: 10.1016/S0140-6736(10)60751-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Ludwig DS, Rouse H, Currie J. PLoS Med. 2013;10:e1001521. doi: 10.1371/journal.pmed.1001521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Del Bono E, Ermisch J, Francesconi M. J Labor Econ. 2012;30:657–706. [Google Scholar]
- 87.Hsin A. Demography. 2012;49:1385–1405. doi: 10.1007/s13524-012-0123-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.